Social Activities Structured play
Social Activities Structured play





Structured play can be a good way for children with autism spectrum disorder (ASD) to learn play skills like sharing, taking turns and being with other children.
How autism spectrum disorder can affect play
Children with autism spectrum disorder (ASD) enjoy playing, but they can find some types of play difficult. It’s common for them to have very limited play, play with only a few toys, or play in a repetitive way. For example, your child might like spinning the wheels on a car and watching the wheels rotate, or might do a puzzle in the same order every time.
Because ASD affects the development of social skills and communication skills, it can also affect the development of important skills needed for play, like the ability to:
- copy simple actions
- explore the environment
- share objects and attention with others
- imagine what other children are thinking and feeling
- respond to others
- Take turns.
How structured play can help children with autism spectrum disorder
Structured play is when a grown-up provides resources, starts play or joins in with children’s play to offer some direction or guidelines. Free play is unplanned play that just happens, depending on what children are interested in at the time. Both are both important for children’s development, but structured play activities are particularly useful for children with autism spectrum disorder (ASD) who are learning early play skills like sharing, taking turns and interacting with other children.
This is because a structured play activity usually gives children clear guidelines about what to do and when. It also usually has a clear end point. This reduces the number of options that can come up in a play scenario, which can sometimes be overwhelming for children with ASD. A clear structure can also help your child understand the steps, skills, activities or ideas that are needed to get to the end goal of the game.
All of this creates a lower-stress environment where your child can practice the skills he needs both to play and interact successfully with other children. Once your child has learned the steps, over time she might be able to start and finish the activity without support.
How to structure a play activity for children with autism spectrum disorder
The first step is choosing an appropriate play activity. Activities that have a clear goal and ending are best, like jigsaws, puzzle books, song and action DVDs, picture lotto and matching games.
Next, you could try creating a visual schedule:
-
- Represent each step of the activity with visual cues attached to a board. The cues could be objects, pictures or words.
- Pull off each cue during the activity as your child progresses, so that you clearly show what the next stage of the activity is.
- Gradually reduce your support until your child can use the schedule and complete the activity on his own.
To start with, your child might not find the activity or its end result fun by itself. You might need to add something else to help your child learn that this type of play can be fun. For example, if your child loves your tickles, you can tickle her after each stage of the activity is finished, and then have a big tickle session at the end of the whole activity. This extra reinforcement will help your child to have a positive experience of the structured play activity while he’s still learning play skills.
Top tips for structured play with children with autism spectrum disorder
These tips can help you and your child with autism spectrum disorder (ASD) gets the most out of structured play:
- Use your child’s interests. For example, if your child loves Thomas the Tank Engine, start by using Thomas-themed jigsaws, puzzles or colouring books.
- Choose activities that your child can do. Think about what stage your child is at and try moving play onto the next stage. For example, if she’s banging blocks, introduce some turn-taking with the blocks
- Use your child’s strengths. For example, if your child responds well to visual cues, try a very visual activity like sorting coloured blocks.
- Talk only as much as you need to.
- Keep playtime short.
- Redirect inappropriate play. For example, if your child is banging blocks together, you could prompt him to stack them, or redirect him to an activity that involves banging.
Developing Play
As your child with autism spectrum disorder (ASD) becomes more able to complete structured play activities on her own, you can begin to expand how long you play and the number of activities you do with your child. For example, once your child can complete a few activities, try to set up a few different play stations around the house. This way, your child can practice moving between activities and focusing on different things without having you there all the time.
Structured play groups help students develop their play and social engagement skills. They involve carefully chosen play activities which encourage peer interaction and build social and communication skills. The groups normally include a balance of students with social support needs and typically developing peers who can act as models. Activities and materials used are carefully selected to foster interactive play and skill building is supported by teachers and other adults.
How do I use it?
- Identify no more than two students with social support needs.
- Select two or three peers who are good at socialising, are helpful to others and able to follow adult direction well.
- Identify no more than two goals for the group e.g. the student will learn turn-taking while interacting with peers in a fun activity
- Select activities for the group e.g. construction or dramatic play activities that match the interests of the students
- Collect the necessary materials for the activity
- The play session should last no longer than 30 minutes.
- Implement the play group at appropriate times e.g. during whole class free play or group activity times. The adult/teacher helps scaffold the play, offering advice or direction when needed.
Getting Started (Activity or Event)
What important events or activities tend to set up the behaviour?
When the individual experiences or is engaged in one of the following:
- Is in the community
Out on an excursion with the school, out shopping, attending a club, playing or attending a sporting activity - Has recently been disciplined
Has been reprimanded for an action or behaviour, has had something important confiscated as a consequence of an action or behaviour. - Is engaged in an activity or task they dislike
Has been asked to complete a non-preferred task or activity. - Is eating
- Is working in a group
Small group Maths or English lesson, social skills group, unmonitored small group learning such as independent reading groups. - Is working independently
Has been asked to complete a task on their own without assistance. - Is in a regular class
Is working with the rest of the class in the classroom in a standard lesson (e.g. Maths, English) - Is playing
Is playing inside or outside during a scheduled break, is engaged in free time in class, this could be structured or unstructured, alone or with others. - Is returning to school after a break
Has returned after a holiday or a public holiday, after being sick, after a suspension. - Has had a change in routine
Has a relative visiting, has a relief/ new teacher, doctor/ dentist appointment. - Is attending a special event
At school- Sports Day, Anzac Day Parade, and incursion. At home- a friend’s birthday, a sporting event. - Is in a specialist lesson
Music, PE and Art - Is transitioning between activities or settings
Transitioning can refer to moving from one classroom to another, one classroom activity to another or from an activity to playtime or lunch. It can also refer to moving from the playground to lining up or getting out of the car to go into the classroom. Therefore a transition is any moment in time where the individual is required to move from one area or activity to another. It is important to recognise that some people may be more or less sensitive to the changes between activities, locations or people, so although you may feel that the change was minimal (e.g. moving from working on their desk in the class to working on a desk in the library), this may feel more significant to somebody else. Other examples include moving between classes, from class to lunch, home to school, home to job or starting a new class or school year. - Is unwell or tired
This may be identified by the individual or others who know them.
What happens before
What happens to set off the problem behaviour? Often it’s when someone..
- Directs them to start or continue with a disliked task
Directs individual to start or continue with a non-preferred task or something that the individual finds difficult or uncomfortable. - Directs them to stop a liked task
Asks them to stop an enjoyable activity or task. - Does not respond to their approach
Individual does not respond to another person’s approach and continues with the behaviour or activity e.g. does not notice them trying to gain attention, does not stop talking to another person when approached. - Does not respond to their request
Individual does not respond to another person’s request e.g. does not answer a question or join in with an activity - Gives a physical prompt
Individual is given a physical guide to complete a task or reengage with an activity e.g. touches person, or taps them on their arm or shoulder to gain their attention or guides their hand towards the task. - Gives a verbal direction or request
Somebody says a direction or request to the individual. This may be directly to the individual or to a group of people. - Gives verbal praise
Verbally praises the person for something, either about the person themselves or something they have said or done e.g. “good job” or “you did really well in that sport lesson”. This may be directly to the individual or to the whole class. - Gives a verbal reminder
Somebody reminds the individual of something by saying it to them e.g. “it’s time to get in the car”, “go back to class”, “brush your teeth”, “don’t forget to pack your lunch”. This may be directly to the individual or to a group of people. - Gives a verbal reprimand
Tells individual off, possibly for doing something or saying something . - Makes an unexpected noise or sound
Person or people nearby make sudden noise or sound such as a hand clap or shouting . - Moves away
Moves away from the person intentionally or unintentionally. - Moves closer
Moves closer to the person intentionally or unintentionally - Refuses a request
Refuses to do something or let the person do something
What happens after
What happens as a result of the individual engaging in this behaviour?
The individual is then:
- Given a verbal redirection to stop the behaviour
The individual is given a spoken instruction which has the aim of stopping the behaviour and directing them towards a more acceptable behaviour e.g. “Chairs are for sitting. No standing please” . - Given more information or clarification of the direction or request
Clarify and simplify the expected task. Break it into one or two steps at a time. Make the directions explicit. - Allowed to remain with preferred task or activity
Is allowed to continue with the an activity or task they enjoy or would chose. - Reminded of the rules and consequences
Is reminded of house, school or workplace rules and the consequences that follow if the rules are broken. - Asked the Responsible Thinking Questions
Responsible thinking questions allow the individual to make choices about their actions. E.g. What are you doing? What are the expectations? What happens when you ignore these expectations? Is this your goal? What do you want to do now? - Given a forced choice
Instead of telling the individual what to do, options are presented as a choice e.g. “do you want to do your Maths or English homework?” or “If you don’t complete this activity now you are choosing to finish it at break time” - Ignored
Others do not respond to the behaviour, either purposefully or not. - Given attention by peers
Peers watch on, join in or encourage the behaviour (this may be positive or negative attention). - Given 1:1 attention from adult
An adult directs their attention to the individual exhibiting the behaviour. This may be positive or negative attention, and would include things like speaking to the individual to tell them that their behaviour is wrong or sitting with the individual to encourage them to complete a task. - Given reduced task demands
Individual is given a section of the task to complete instead of all of the task. - Redirected to a different task or activity
Individual is directed to a different task. - Isolated
Individual is removed from the area where the behaviour has occurred or the people around the individual are removed from the area. - Sent to another area
Individual is directed away from the location they were when the behaviour occurred, this would include being sent out of the class or to a safe zone.
Problem Behaviour
What does the problem behaviour look like?
The individual:
- Is off task but remains seated in appropriate area
Is not participating in the requested task but is not moving around the room. - Is off task and distracting other students
Is not participating in the requested task and is disturbing others by moving around or being noisy - Does not respond to direction or request
Will not follow directions. Ignores requests. - Leaves their seat without permission
Gets up and moves around the room they are in when it may not be appropriate. - Makes repetitive requests or sounds
Repeats questions or sounds, may be distracting for those around. - Verbally refuses or rejects directions or request
This may be with words (e.g. “no”, “go away” or other sounds in response to being asked to follow a direction. - Becomes verbally abusive
This may be noises, single words or phrases e.g. shouting or swearing. - Becomes physically aggressive
Becomes physically aggressive towards the person or people around them e.g. hits, bites, throws objects, moves furniture or physically attacks another person. - Destroys property
Breaks or damages property around them (this may include their own possessions or ripping up pieces of work).
Desired Behaviour
What do you want to see them doing instead?
- Follow the direction
Individual follows the direction given and participates in the activity requested. - Start task
Individual starts or attempts task after a suitable amount of take up time. - Stop task
Individual stops the task. - Acknowledge the reminder
Verbally or non-verbally acknowledge that they have been given a reminder - Acknowledges the praise
Individual acknowledges the praise verbally or non-verbally. - Work quietly
Work quietly without distracting others individuals from their own work - Tolerate light brief touch
Individual is able to accept a light brief touch, which may be for a redirection, reminder or attention getter or may be due to somebody witting in the close vicinity. - Ask person to move away or closer
Individual is able to verbally or non- verbally request that a person moves closer to them or away from them. - Ask for help
Individual is able to ask another person for assistance verbally or non-verbally. - Ignores interruption or noise
Individual continues to work without reacting to interruption or noise. - Repeats request or question
Individual repeats the request or question for clarification. - Accepts refusal
Individual accepts that their request cannot be fulfilled, e.g. not allowed access to an activity or object they have requested.
Consequence
What will happen when the individual displays the desired behaviour?
- Provide tailored adult attention
Give the individual some specific adult attention e.g. some positive feedback. - Given additional time of preferred activity
Individual is given some extra time on their preferred activity after the task is complete. - Verbal acknowledgement of compliance or success
Praise or positive feedback. This may need to be done without anyone around the individual hearing. - Assign free time or choice of preferred activity
Give individual a designated amount of time later in the day to engage in a preferred activity. - Offer choice of tasks or scheduling of tasks
Give the individual a limited amount of predesignated choices of activity, or allow them to choose when they have to complete the task
Acceptable Alternative
What behaviour would you accept as an alternative while teaching the desired behaviour?
- Ask for help
Lets someone know that they require help (verbally or non-verbally). - Tell adult they are uncomfortable
Lets an adult know they are feeling uncomfortable (verbally or non-verbally). - Politely decline
Lets the other person know that they do not want to join in the new activity. - Accepts the reminder
Individual accepts the reminder and moves to the task after a period of take up time. - Go to pre-arranged safe space
Moves to pre-arranged safe zone such as a tent or quiet corner in the classroom, support room or buddy class. At home, this may be their bedroom. - Works on alternative task
Works on a task other than the one set, which may or may not be related to the initial task assigned. This may be one the individual has identified or may be one set by the adult. - Waits quietly for assistance
Waits without interrupting other individuals. Possibly engaged in pre-arranged quiet activity.
What is the function, or reason, for the behaviour?
People engage in millions of different behaviors’ each day, but the purpose or “functions” of these different behaviors’ tend to fall into the categories listed below. Remember: once the function has been met the problem behavior should stop. If it doesn’t stop then you haven’t identified the correct function and you will need to revisit the information you have entered. This is a good result – the more functions you rule out the closer you will get to the true function.
These functions are to either get access to, or to stop/avoid:
- Stimulation or sensation: This could be escaping from a sensation that is unpleasant (such as a noisy hall or flickering light) or accessing something that is enjoyable. Remember, everybody has different sensory preferences, so what is normal or enjoyable for one person may be uncomfortable or distressing for another.
- An item or activity: This could be escaping or avoiding an activity or task that is difficult or not enjoyable, or gaining access to a favourite or preferred item or activity (e.g. access to technology).
- Social situation with child: This could be any behaviour to get or stop focused attention from siblings, peers, or other children that are around them. Remember, whilst some individuals find attention from other children positive, others will find it unpleasant and will therefore show behaviours to try and make it stop.
- Social situation with adult: This could be any behaviour to get or stop focused attention from parents, teachers or other people that are around them. Remember, being disciplined and told-off might sometimes be a form of gaining engagement from adults.
With this information in mind, take some time to look through the diagram that you have completed and think about what changed as a result of the behavior. Remember, use the information in the diagram to inform you; sometimes the function of behaviors’ can surprise people!
ABA-Applied Behaviour Analysis
ABA-Applied Behaviour Analysis




ABA-Applied Behaviour Analysis
Behavior analysis is a scientifically validated approach to understanding behavior and how it is affected by the environment. In this context, “behavior” refers to actions and skills. “Environment” includes any influence – physical or social – that might change or be changed by one’s behavior.
On a practical level, the principles and methods of behavior analysis have helped many different kinds of learners acquire many different skills.
What is Applied Behaviour Analysis?
 Behavior analysis focuses on the principles that explain how learning takes place. Positive reinforcement is one such principle. When a behavior is followed by some sort of reward, the behavior is more likely to be repeated. Through decades of research, the field of behavior analysis has developed many techniques for increasing useful behaviors and reducing those that may cause harm or interfere with learning.
Behavior analysis focuses on the principles that explain how learning takes place. Positive reinforcement is one such principle. When a behavior is followed by some sort of reward, the behavior is more likely to be repeated. Through decades of research, the field of behavior analysis has developed many techniques for increasing useful behaviors and reducing those that may cause harm or interfere with learning.
Applied behavior analysis (ABA) is the use of these techniques and principles to bring about meaningful and positive change in behavior.
These techniques can be used in structured situations such as a classroom lesson as well as in “everyday” situations such as family dinnertime or the neighborhood playground. Some ABA therapy sessions involve one-on-one interaction between the behavior analyst and the participant. Group instruction can likewise prove useful.
How Does ABA Benefit Those with Autism?
 Today, ABA is widely recognized as a safe and effective treatment for autism. In particular, ABA principles and techniques can foster basic skills such as looking, listening and imitating, as well as complex skills such as reading, conversing and understanding another person’s perspective.
Today, ABA is widely recognized as a safe and effective treatment for autism. In particular, ABA principles and techniques can foster basic skills such as looking, listening and imitating, as well as complex skills such as reading, conversing and understanding another person’s perspective.
That ABA techniques can produce improvements in communication, social relationships, play, self care, school and employment. These studies involved age groups ranging from preschoolers to adults. Results for all age groups showed that ABA increased participation in family and community activities.
A number of peer-reviewed studies have examined the potential benefits of combining multiple ABA techniques into comprehensive, individualized and intensive early intervention programs for children with autism. “Comprehensive” refers to interventions that address a full range of life skills, from communication and sociability to self-care and readiness for school. “Early intervention” refers to programs designed to begin before age 4. “Intensive” refers to programs that total 25 to 40 hours per week for 1 to 3 years.
These programs allow children to learn and practice skills in both structured and unstructured situations. The “intensity” of these programs may be particularly important to replicate the thousands of interactions that typical toddlers experience each day while interacting with their parents and peers.
Such studies have demonstrated that many children with autism experience significant improvements in learning, reasoning, communication and adaptability when they participate in high-quality ABA programs. Some preschoolers who participate in early intensive ABA for two or more years acquire sufficient skills to participate in regular classrooms with little or no additional support. Other children learn many important skills, but still need additional educational support to succeed in a classroom.

COGNITIVE BEHAVIORAL THERAPY
Cognitive Behaviour Therapy




COGNITIVE BEHAVIORAL THERAPY.
Cognitive Behavioral Therapy (CBT) is a talking therapy that can help people to manage their problems by changing the way they think and behave.
CBT is designed to help people notice and understand how their thoughts, behaviors’ and emotions affect each other. It is also designed to help them learn new ways of thinking about and responding to distressing situations.
The therapist breaks down problems into feelings, thoughts and actions to work out which are unhelpful or unrealistic. The therapist then teaches the client how to replace those feelings, thoughts and actions with more helpful and realistic ones.
There are numerous interventions for people on the autism spectrums which are based on, or which incorporate, the principles of CBT.
These include multi-component CBT programmed such as Behavioral Interventions for Anxiety in Children with Autism; Exploring Feelings; and Facing Your Fears.
BEYOND BEHAVIOUR
Therapies based on the science of behavior have been effective for people of all ages, and are an essential item in any mental health professionals toolkit. They only go so far, however. Human beings are “meaning makers.” That is, their behavior is not just the result of stimulus and response or reward and punishment. They take in what is happening around them and give it meaning, loaded with emotion. Then they behave.
CBT takes into account the thoughts (or cognitions) we have about things, the feelings that result, and the behavior that follows.
CBT: A POWERFUL APPROACH
ADAPTING CBT FOR ASD
In recent years, there have been a number of attempts to adapt CBT for children and teens on the autism spectrum. The focus has often been on those who also have anxiety because this is so common in individuals with ASD.
One challenge was to find out whether children with ASD have the skills necessary to succeed at CBT. Fortunately, it appears they do. A study published in 2012 evaluated the cognitive skills of children with ASD and compared them to those of typical children. The children with ASD had the skills required for CBT in almost every instance. They were able to distinguish thoughts, feelings, and behaviors, and to work on altering their thoughts. Their only area of difficulty was in recognizing emotions.
In addition, traditional CBT tends to require strong linguistic and abstract thinking abilities, and these can be a challenge for individuals on the autism spectrum. Realizing this, researchers have worked to develop modifications to CBT that render it more ASD-friendly, such as making it more repetitive, as well as visual and concrete.
 For example, instead of merely asking children to verbally rate their anxiety on a scale of 1 to 10, the therapist might have a thermometer showing anxiety from low to high and have the participants point to the prop to illustrate how high their anxiety is around a certain situation. Another strategy is to focus on the children’s talents and special interests, which helps keep them engaged and motivated, and to build in frequent movement breaks or sensory activities for those who might have problems with attention or sensory under- or over-reactivity.
For example, instead of merely asking children to verbally rate their anxiety on a scale of 1 to 10, the therapist might have a thermometer showing anxiety from low to high and have the participants point to the prop to illustrate how high their anxiety is around a certain situation. Another strategy is to focus on the children’s talents and special interests, which helps keep them engaged and motivated, and to build in frequent movement breaks or sensory activities for those who might have problems with attention or sensory under- or over-reactivity.
CBT can be delivered in a variety of ways: individual, family, group, or even family and group. The advantage of group CBT is that individuals with ASD learn that others are struggling with the same issues, and they begin to overcome them together. Friendships and social support gained through this process may be healing in themselves.
The advantage of family CBT is that it involves parents, educating them about their child’s challenges and teaching them to encourage use of CBT techniques when real life situations confront their child. This can make them feel more hopeful and confident in their ability to contribute to positive change in their child’s life.
However it recommended that CBT might be appropriate as a treatment for anxiety and depression in many adults on the autism spectrum, as this is in line with existing guidance for those disorders, provided those programmes are modified to meet their specific needs.
It also reported that there is insufficient evidence to determine if CBT is an effective treatment for other coexisting mental health disorders (such as depression) in children on the autism spectrum. However it recommended that CBT could be used for the treatment of those disorders in children on the autism spectrum, as this is in line with existing NICE guidance for those disorders.
Our Opinion
- There is a reasonable amount of high quality research evidence to suggest that multi-component CBT programmes may help reduce the symptoms of anxiety in some primary school children and adolescents on the autism spectrum who have an IQ of 70 or more.
- There is insufficient evidence to determine whether CBT programmes can help any child or adult on the autism spectrum with other issues, such as anger or depression.
- There is insufficient evidence to determine whether CBT programmes can help people with the core features of autism.
- There is insufficient evidence to determine whether CBT programmes can provide any benefit to adults on the autism spectrum.”
- Carrying out a detailed assessment of the individual, including any key strengths and weakness.
- Modifying the therapy to take account of the needs of that individual, including any strengths and weaknesses.
- Use of a longer assessment phase and an increased number of treatment sessions to help the initial engagement with the therapist, to enhance emotional literacy, and to practice, consolidate and generalise the techniques learnt.
- Using a range of appropriate measures to evaluate the effectiveness of the therapy.

Parental Counselling
Brain Gym Exercises

Psychological counselling for slow learner, parental guidance and counselling.
As parents, looking after ourselves is something that seems to get put way down the list of priorities. Everything and everyone are somehow organized, nurtured and sorted out irrespective of how we may be feeling. If life appears to be getting out of control or you’re not coping so well, don’t think you have to manage it alone. The old adage ‘a problem shared is a problem halved’ has truth in it, and there are plenty of professional services which can help you in a time of need.
School counselors
When there is an issue in some way related to school that is affecting the whole family, school counselors are a great place to go for help. School counselors are experienced teachers who have formal qualifications in counseling. They are available for all students from preschool to Year 12, and their families. As with any professional service, they will keep information confidential, unless child protection legislation overrides it or where someone may suffer serious harm from information being withheld.
Face-to-face support
Your doctor is a good person to approach initially for some advice or assistance if life is getting out of hand. If you need further support, your doctor can provide you with a referral to a psychologist or another other type of counselor. However, if you want to find a psychologist yourself.
What is Child Counseling?
 Child counseling is a specialized area of psychology focused on working with children who have a mental illness, have experienced a traumatic event, or are facing a difficult family situation. Child counseling often deals with many of the same issues that adults do, such as anxiety or grief, but this type of therapy focuses on breaking these problems down so that children can understand and make sense of them.
Child counseling is a specialized area of psychology focused on working with children who have a mental illness, have experienced a traumatic event, or are facing a difficult family situation. Child counseling often deals with many of the same issues that adults do, such as anxiety or grief, but this type of therapy focuses on breaking these problems down so that children can understand and make sense of them.
Child counselors are specialists who can offer insight into the inner workings of your child’s development that are not necessarily visible to even those closest to the child. Most important of all, your child may not be able to tell you what sort of help they need, so your judgment is critical in ensuring your child receives the therapeutic intervention that is best for them.
Child Counseling can help kids interpret issues in a way that they can understand. Child counselors and therapists are highly trained in the thought processes of children so they can help kids and youths to interpret issues or trauma in a way that they can understand. When a child’s emotional issues are left untreated, it’s likely that they’ll impact the child’s educational and development and can also persist into adulthood.
Children of all ages can attend counseling sessions, from young preschoolers to teenagers. Every age within this range falls into the realm of child counseling until they are adults and no longer need children’s counseling techniques. Child counseling aims to help children work through their emotions so they can live normal healthy lives without fear, confusion, anxiety or trauma in their lives.
Why Seek Child Counseling?
When dealing with the mental and emotional health of your young child, sometimes the guidance of a professional can illuminate the underlying issues your child is experiencing. Many children are unable to express the complexities of having emotional or mental problems, so counseling can be an excellent option to explore the causes of your child’s issues.
In many cases, children who have a mental illness such as obsessive-compulsive disorder, post-traumatic stress disorder, or general anxiety disorder. Parents and physicians may seek the services of a child counselor to help determine a diagnosis, or counseling may be part of a key part of a treatment plan for mentally ill children. Child counseling unites your concerns with the knowledge of a therapist who has the tools and experience to help your child through difficult times. Parents want the best for their children, but the situation may be too challenging to handle on your own, especially as you are emotionally involved. When you seek child counseling, a third-party professional can help your child with strategies that are designed with their well-being in mind, first and foremost.
Issues Addressed by Child Counseling
If your child has experienced tragic or unsettling events in his or her life, such as the unexpected loss of a loved one or an abusive episode, the stress of the situation may be difficult for them to understand. Some of the most common issues that child counseling addresses are:
- Divorce
- Death of a loved one and grief
- Witnessing or experiencing a trauma
- Mental health diagnoses, including anxiety and depression
- Bullying
- Sexual, emotional, or physical abuse
- Relocating schools or cities
- Substance abuse or addiction in the family
Signs Your Child May Need Counseling
A child who displays developmental problems or acts out in ways that are beyond what’s considered normal can likely benefit from counseling, especially if there has been a recent trauma or significant event that impacts their lives, like a death or divorce. Some of the signs that your child is in distress and could need counseling include
- Unwarranted aggression
- Incontinence
- Difficulty adjusting to social situations
- Frequent nightmare and sleep difficulties
- Sudden drop in grades at school
- Persistent worry and anxiety
- Withdrawing from activities they normally enjoy
- Loss of appetite and dramatic weight loss
- Performing obsessive routines like hand washing
- Expressing thoughts of suicide
- Talking about voices they hear in their head
- Social isolation and wanting to be alone
- Alcohol or drug use
- Increased physical complaints despite a normal, healthy physician’s report
- Self-harm such as cutting
Goals of Child Counseling
Child counseling addresses major issues in a child’s life with the intended outcome being that they can learn tools to deal with stress or trauma. Some of the common goals of child counseling include being able to cope with difficult situations such as:
 Anxiety:
Anxiety:
Children who attend counseling are encouraged to learn techniques to deal with emotional distress and anxiety on their own. Children can learn to prevent panic attacks or cope with anxiety in a variety of ways, which they will learn in their counseling sessions. Some strategies they will learn may include breathing exercises, changing negative self-talk, muscle relaxation, talking to a trusted adult about their feelings instead of keeping them inside, and asserting themselves by knowing when to remove themselves from a stressful situation. Teaching these techniques to children gives them a toolbox of coping mechanisms that they can use when they become anxious or experience a panic attack.
Trauma:
Unfortunately, some children experience traumatic events and are exposed to disturbing situations that they should not have to witness or be part of. After a trauma, a child may experience shock, disbelief, detachment or emotional numbness, fear, and may develop post-traumatic stress disorder. Symptoms of PTSD include strong desire to avoid the people or places where trauma was involved, vivid and distressing memories or flashbacks, nightmares or insomnia or fear of going to sleep, and being easily angered or agitated. Child counseling aims to help children talk about the trauma that they faced, rather than keeping their experiences and emotions inside. Many children who experience trauma develop trust issues and may have a difficulty finding the words to express their feelings and may blame themselves for what happened.
Child counseling teaches children that it’s okay to talk about their experiences and that they can use a variety of coping mechanisms. When a child has a flashback to their trauma, child counselors teach them tools such as deep breathing, seeking out an adult to talk to, relaxing their muscles, and correcting the misinterpretation of traumatic events.
Divorce:
When a marriage dissolves, it can be very challenging for children in the family to cope with. Many children blame themselves for their parents splitting up or have feelings that they are unloved. With divorce often comes changes in custody, and in some cases, there are tense custody battles between parents. Children can feel guilty about choosing which parent they want to live with and feel distress if their choices or feelings don’t align with their siblings. Child counseling teaches children to deal with feelings of sadness, fear, and guilt by giving them techniques to use such as deep breathing, journaling or art therapy, practicing positive self-talk, and talking about their feelings with their parents or another trusted adult.
Grief:
A death of a loved one, whether it’s a family member, peer, or friend of the family is distressing for anyone; however, children often cannot cope with death in the same way that adults can. For children, it may be difficult to understand their feelings of loss, despair, sadness, and missing the person who died. Often, children may have irrational thoughts such as the fear that they will also die, thinking that the death was their fault, or believing that they could have prevented it. Child counseling helps children understand the grieving process and teaches them that it’s okay to experience the emotions that arise after losing a loved one. Coping strategies may include being able to talk about their feelings, channeling grief through creative pursuits like journaling or art, and allowing themselves to speak or think about their loved one through sharing personal memories. Teaching children the stages of grief is another technique that helps them understand that how they feel is normal and natural.
Significant Change:
For many children, events, like moving to a new city or changing schools, can be stressful. Many adults can accept these changes as part of life, so you may not realize the impact it has on your child. Children who have difficulty dealing with change can experience feelings of insecurity, anxiety or worry, or anger towards their parents. While these are normal reactions to significant change, many children have a hard time moving past these feelings on their own. Child counseling teaches children to cope with change through learning to focus on the positive and stable aspects of their life, positive self-talk, deep breathing exercises when anxiety arises, and understanding that change is natural, understanding that their feelings are temporary and will fade when they adjust to the situation.
Self-Esteem and Confidence
Many children struggle with poor self-esteem and low confidence which can lead to depression, substance abuse, eating disorders, or thoughts of self-harm. When a child has poor self-esteem, they may feel unloved, worthless, and their friends and family would be better off without them. Child counseling can help children improve their self-esteem in a variety of ways, including digging deeper into underlying issues that may have caused these beliefs, recognizing negative self-talk and turning it into positive thoughts, using affirmations to gain confidence and self-acceptance, and talking to a trusted adult when troubling feelings arise. If a child’s low self-esteem has developed into something more serious, like an eating disorder, child counselors are equipped to help children overcome those issues.
Types of Child Counseling
Cognitive-behavior therapy (CBT):
CBT focuses on helping children change negative styles of thinking and behaving by correcting or re-purposing the thought process toward a more positive response. CBT challenges the automatic internal beliefs a child has about themselves and teaches them to view themselves and their situation through a more realistic and positive lens. CBT provides children with practical tools for coping with difficult or stressful situations that they can learn to use on their own.
Trauma-Focused CBT (TF-CBT):
TF-CBT is designed to help children overcome the effects of trauma. As with traditional CBT, children are taught to see events more realistically without blaming themselves. TF-CBT teaches children strategies that they can use when they experience a flashback so they can work through the memories from a place of control and understanding, and gives them the ability to use these tools on their own.
Alternative Therapies:
Children respond well to alternative types of therapies like art therapy, music therapy, movement therapy, equine therapy, mindfulness, or aquatic therapy.

What to Look for in a Child Counselor?
 When seeking a counselor for your child there are several considerations to keep in mind. First and foremost, a child counselor must be a good fit for your child.
When seeking a counselor for your child there are several considerations to keep in mind. First and foremost, a child counselor must be a good fit for your child.  Chances are, your child will be uncomfortable with their initial counseling sessions, but it’s important that they work with a therapist that they are a good interpersonal match with. If your child is not comfortable with their counselor after several sessions, you may consider looking for another person who is a better personality fit for your child. Another important consideration is what the counselor’s training and qualifications are. It’s imperative to use a counselor who specializes in child counseling so they can apply therapy techniques to a young mind. Since you’re dealing with your child’s mental well-being, don’t hesitate to check references, credentials, and meet with a potential therapist to gauge your comfort level. Often therapists offer free consultations in which they can explain how beneficial counseling will be for your child
Chances are, your child will be uncomfortable with their initial counseling sessions, but it’s important that they work with a therapist that they are a good interpersonal match with. If your child is not comfortable with their counselor after several sessions, you may consider looking for another person who is a better personality fit for your child. Another important consideration is what the counselor’s training and qualifications are. It’s imperative to use a counselor who specializes in child counseling so they can apply therapy techniques to a young mind. Since you’re dealing with your child’s mental well-being, don’t hesitate to check references, credentials, and meet with a potential therapist to gauge your comfort level. Often therapists offer free consultations in which they can explain how beneficial counseling will be for your child
Parents can help their children with the school year transition through considering the following points:
- Communicate.
The most important tool for easing the back-to-school transition and helping children manage their stress is communication. Keeping an open channel of parent-child communication is key. Children should feel free to talk about their hopes and their disappointments, their successes and failures, their joys and their anxieties, all with the confidence that their parents can handle whatever they hear and will respond without undue anxiety or reproach. Accept whatever your children are feeling and then move on to helping them learn how to cope. Remember also that such communication should not be a one-time event, but rather on ongoing conversation. - Anticipate.
Communication about the start of the school year should begin before the event itself. Beginning in mid- to late-August, parents should begin the conversation about the beginning of school and its possible stresses by asking their children about what they anticipate in the coming year…academically, socially, and in terms of athletics, dance or other extra-curricular activities. In their own words, parents might ask their children what they hope for and is there anything that they fear? What are they looking forward to and what do they worry about? - Age Matters.
How we talk with our children and what they hope for and fear differs greatly by their ages. We ask simpler questions and expect to be more active in helping young children cope. We are careful to emphasize strengths and not to be intrusive with our early teens. However, we can be more direct and appreciate the considerable capabilities of our 16 to 18 year olds. - Complexity Matters.
We must also consider the complexity of our children’s school experience. They face not only academic challenges and accomplishments but also complex social relationships, both with peers, adult teachers and administrators. Our children see ample examples of kindness and caring in school, but also copious amounts of meanness and bullying. They are called on to perform publicly, day in and day out, reading, doing math, taking part in class debates, and in gym class. Our children face a complex cultural landscape as well as they join classmates of different races, ethnicities, and religions, some native born and some immigrant, some homosexual and some heterosexual, all in a nation-wide political context that emphasizes division and recrimination. Parents should take an active role in learning about the many roles and relationships their children are involved in at school and offer to help them navigate any complexities that arise. - Normalize.
When Appropriate. The beginnings of new experiences are often hard, at school, at work, in relationships, and in community activities. It is normal for children to have fears and it is normal for transitions to be rough. Letting our children know that this is so and that we have faith in their ability to cope is a good foundation for subsequent action. - Coping Rather than Protection.
Many parents understandably have the desire to solve their children’s problems, to make it all better. However, this does not take full advantage of the opportunity that helping with school transitions offers. It is better to have a conversation with our children about how they can cope, how they can manage the academic challenges and the social strains, than to take care of these issues ourselves. Coaching our children on how to cope will bring benefits that last far longer than solving their problems for them. - Coping Tool Box.
One way to talk with your child about how he or she can cope is to conceptualize this as a coping toolbox. You can discuss both what tools he or she already has, such as reaching out to an adult, and methods that are new to them, such as using calming thoughts or remembering times when they have been successful. - Teachers Are Our Allies.
Finally, I encourage parents to remember that teachers care about our children’s well-being nearly as much as we parents do. Reaching out and talking with our children’s teachers’ – letting them know how our children are feeling, listening to the teachers’ perspective, and enlisting their help when appropriate, goes a long way both to solving problems and letting our children know that many people care about them.
What is Child Therapy/Child Counseling?
 Child therapy (also called child counseling) is much the same as therapy and counseling for adults: it offers them a safe space and an empathetic ear while providing tools to bring about change in thoughts, feelings, and behaviors.
Child therapy (also called child counseling) is much the same as therapy and counseling for adults: it offers them a safe space and an empathetic ear while providing tools to bring about change in thoughts, feelings, and behaviors.  Just like adult clients, child clients receive emotional and goal support in their sessions. They may focus on resolving conflict, understanding their own thoughts and feelings, or on coming up with new solutions to problems.
Just like adult clients, child clients receive emotional and goal support in their sessions. They may focus on resolving conflict, understanding their own thoughts and feelings, or on coming up with new solutions to problems.
The only big difference between adult therapy and child therapy is the emphasis on breaking down mental illness, trauma, or any other difficult issue the child is dealing with, to ensure children understand what is happening and can make sense of what they are experiencing.
Child therapy can be practiced with one child, a child, and a parent or parents, or even with more than one family. It is often administered by a counselor or therapist who specializes in working with children, and who can offer the parents and/or guardians insights that may not be immediately apparent.
The therapist and client(s) can cover a wide variety of issues and problems in counseling, including:
- Divorce or separation
- Death of a loved one
- Witnessing or experiencing a trauma
- Bullying
- Sexual abuse
- Emotional abuse
- Physical abuse
- Family or child relocation
- Substance abuse or addiction in the family
- Mental illness, like depression, anxiety, and obsessive-compulsive disorder
Whatever the treatment is sought to alleviate or address, it will likely be very forward-oriented (meaning there will be little looking back or digging up the past) and will probably be conducted in a non-verbal manner for a large portion of the time (including play, games, art, etc.).
In addition, the therapy sessions may focus on five important goals on top of any situation-specific goals:
- Building the child’s self-esteem
- Helping to improve the child’s communication skills
- Stimulating healthy, normal development
- Building an appropriate emotional repertoire
- Improving the child’s emotional vocabulary
To summarize, child therapy is quite similar to therapy for adults in terms of the purpose, goals, and problems it can address, but it narrows the focus to issues that young children struggle with and emphasizes a future-oriented perspective, along with including techniques and exercises that are appropriate for the child’s age.
When is Child Therapy Effective?
As noted above, child therapy can be effective for a wide range of issues. If a parent is not sure whether the child needs counseling or not, the list of symptoms below can be a good indicator. If the child is experiencing one or more of these symptoms, coupled with the parent’s concern, it’s probably a good idea to take him or her in for an evaluation.
The following are symptoms that may indicate a problem that child counseling can correct or help with:
- Unwarranted aggression
- Incontinence
- Difficulty adjusting to social situations
- Frequent nightmare and sleep difficulties
- A sudden drop in grades at school
- Persistent worry and anxiety
- Withdrawing from activities they normally enjoy
- Loss of appetite and dramatic weight loss
- Performing obsessive routines like hand washing
- Expressing thoughts of suicide
- Talking about voices they hear in their head
- Social isolation and wanting to be alone
- Alcohol or drug use
- Increased physical complaints despite a normal, healthy physician’s report
- Self-harm such as cutting.
In addition to these issues, the child may be dealing with:
- Persistent feelings of sadness or hopelessness
- Constant anger and a tendency to overreact to situations
- Preoccupation with physical illness or their own appearance
- An inability to concentrate, think clearly or make decisions
- An inability to sit still
- Dieting excessively or bringing followed by vomiting or taking laxatives
If parents decide to bring their child to therapy, they should be sure to stay engaged throughout the therapy process. Child & Adolescent Psychiatry suggests asking the therapist or counselor the following questions:
- Why is psychotherapy being recommended?
- What results can I expect?
- How long will my child be involved in therapy?
- How frequently will the doctor see my child?
- Will the doctor be meeting with just my child or with the entire family?
- How much do psychotherapy sessions cost?
- How will we (the parents) be informed about our child’s progress and how can we help?
- How soon can we expect to see some changes?
Similarly, there are some suggestions on how to talk to a child about going to counseling. It can be awkward or uncomfortable for both the parent(s) and the child to talk about mental health treatment, but following these tips can help them get through it:
- Find a good time to talk and assure them that they are not in trouble. Listen actively.
- Take your child’s concerns, experiences, and emotions seriously
- Try to be open, authentic, and relaxed.
- Talk about how common the issues they are experiencing may be.
- Explain that the role of a therapist is to provide help and support.
- Explain that a confidentiality agreement can be negotiated so children—especially adolescents—have a safe space to share details privately while acknowledging that you will be alerted if there are any threats to their safety
There are many effective forms of child therapy with evidence to back them up, including Applied Behavior Analysis, Behavior Therapy, Cognitive Behavioral Therapy, Cognitive Therapy, Family Therapy, Interpersonal Psychotherapy, and Organization Training. Younger children may also benefit from Play Therapy, and older adolescents may benefit from Dialectical Behavior Therapy, Group Therapy, or Psychodynamic Psychotherapy,
These therapies may be administered on their own, in combination with other therapies, or as a hodge-podge of techniques and exercises from several different types of therapies. In addition, it may or may not be accompanied by medication, depending on the situation.
One of these therapies may work for a child far better than the others, and the type chosen will depend on the issue(s) the child and family are dealing with. However, like with any form of therapy, it is most effective when everyone involved is on board, supportive, and actively contributing to success.
How an Emotional Child Can Benefit from Kids Therapy
An overly emotional child (or one that struggles with inappropriate emotional expression or emotional dysregulation) may suffer from one or more of a variety of issues, including ADHD, mental illness, anxiety, or even an autism spectrum disorder. Whatever the issue they are facing, child therapy can help them deal with it.
Cognitive therapy is a good choice for emotional children, as it involves reducing anxiety and learning new ideas and new ways to channel the child’s feelings and energy. It will also help him or her to identify their inner thoughts, and try to replace the bad ones with more positive, helpful ones. Applied behavior analysis can help the child learn how to respond to situations in better, more effective ways, and will teach them about rewards and punishments for their behavior. Play therapy is a good choice for younger children with emotional issues since they can act them out through toys or dolls.
The type of therapy and techniques that will work best for the child may also depend on which stage of development they are in; Erik Erikson’s groundbreaking theory on the eight stages of psychosocial development is a commonly recognized and accepted theory and can help differentiate between normal, age-appropriate issues and more troublesome symptoms.
The eight stages are:
-
- Infancy:Trust vs Mistrust. In this stage, infants require a great deal of attention and comfort from their parents, leading them to develop their first sense of trust.
- Early Childhood:Autonomy vs. Shame and Doubt. Toddlers and very young children are beginning to assert their independence and develop their unique personality, making tantrums and defiance common.
- Preschool Years Initiative vs. Guilt. Children at this stage begin learning about social roles and norms; their imagination will take off at this point, and the defiance and tantrums of the previous stage will likely continue. The way trusted adults interact with the child will encourage him or her to act independently or to develop a sense of guilt about any inappropriate actions.
- School Age: Industry (Competence) vs. Inferiority. At this stage, the child is building important relationships with peers and is likely beginning to feel the pressure of academic performance; mental health issues may begin at this stage, including depression, anxiety, ADHD, and other problems.
- Adolescence: Identity vs. Role Confusion. The adolescent is reaching new heights of independence and is beginning to experiment and put together his or her identity. Problems with communication and sudden emotional and physical changes are common at this stage.
The final three stages are not relevant for the purposes of discussing child therapy, but they are listed here if you’re curious:
- Young Adulthood: Love – Intimacy vs. Isolation
- Middle Adulthood: Care – Generativity vs. Stagnation
- Late Adulthood: Ego Integrity vs. Despair
Based on these life stages, we know that it is common for children in early childhood to throw tantrums when they don’t get their way; tantrums alone aren’t reason enough to seek a therapist! However, if someone of school age is still throwing tantrums, it may be time to explore therapy and counseling options.

Memory Development Services
Memory Development Services
11 Ways To Strengthen Memory In A Child With Special Needs
Most people don’t think about the process of remembering until they experience memory loss.
-
- But what if the ability to hold and retrieve memories was never there?
- How do you live life like that?
- How do you learn?
Deficits in short-term memory, long-term memory and memory retrieval are common with neurological conditions such as traumatic brain injury, epilepsy, autism, cognitive impairment and learning disabilities. No two brains are exactly alike, so medical studies have had inconsistent results in identifying memory patterns across these conditions.But what if the ability to hold and retrieve memories was never there?






Brain Development
These are the 11 most useful methods.

-
- Use Procedural Memory Whenever Possible For individuals with cognitive impairment or memory loss. The cornerstone of this program is the use of procedural memory, a type of long-term memory that helps people remember how to do each step of a process. In most cases, procedural memory is more reliable than short-term memory or memories that include emotions.
To teach everything from long division and reading comprehension to self-care and chores. Instead of introducing these tasks as concepts, model of each step and increase the level of participation until the subject is able to do it independently. For example, the subject usually does not understand what he/she is reading, but he/she knows that he/she can take a list of questions and go back through a text to find the answers. And even though he/she may not understand a math problem at first, he can line up the numbers and work out the correct answer, then go back to the problem and apply that answer to the original question. - Make A Schedule: A schedule with words, symbols or pictures is an easy way to develop procedural memory for people of all ages. Daily habits and journaling can compensate for many types of memory impairments.
- Take Lots of Photos: Episodic memory is the feeling of remembering one’s own personal history. This type of memory is what allows us to learn from past experience and predict future events. Most people do not fully develop this sense of “autobiography” until they are at least 5 years old – but with a neurological condition, it takes much longer.we take lots and lots of photos to document our autobiographies. Photograph special occasions and everyday occurrences, happy and sad. We name people, places, dates and events. We turn them into greeting cards and theme-based scrapbooks such as “Nature Walks 2010-2012” and “Roller Coasters 2005-2011.”
- Exercise: Vigorous daily exercise has been demonstrated repeatedly in published medical studies to improve cognitive function and memory. At home try to incorporate cross-lateral exercise into our daily routine to strengthen connections between the left and right sides of the brain. Get moving with yoga, Brain Gym, Bal-A-Vis-X, swimming and bicycling.
- Relax: The stress hormone cortisol is known to alter memories, so relaxation is an important component to maintaining the integrity of memory. Meditation and regular spiritual practice are excellent tools for supporting cognitive wellness.
- Vitamins: Some types of nutrient deficiencies may contribute to memory loss. After consulting with my son’s pediatrician, I started giving him vitamin B-12 and the antioxidant coenzyme Q10. Other nutritional supplements that may help with memory are omega-3 fatty acids and the antioxidants beta-carotene, vitamin C and vitamin E
- Sensory Input: To understand what children is thinking, often follow his/her eyes so that we can see what he/she is seeing, and we watch his/her face for reactions to changes in the sensory environment. We’ve noticed that sounds, smells, colors and textures can cause a forgotten memory to raise to the surface of his/her mind. A few bars of a song will remind of the last time he/she heard that music, and a smell will remind him/her of another place with that same smell. He/she is much more likely to remember something that has a sensory experience attached to it.
- Creative Output: Having a creative outlet such as writing, photography, painting, sculpture, woodworking or jewelry making tends to reduce stress and increase memory retrieval. Make creativity part of the daily routine!
- Repetition Through Stories: Used stories to help children process events. To ask them to state both facts and emotions in each story – he/she has a thick collection of stories now. He/she reads and re-reads, writes and re-writes each one.
- Keep It Simple: Simple concepts are much easier to remember than complex concepts. Break down large ideas into smaller chunks that can be stored in long-term memory.
- Make It A Game:Memory games and exercises have been around for centuries because they really work. A game does not have to be complicated or expensive – it can be as simple as a treasure hunt or I Spy at home – but it should always be fun!
- Use Procedural Memory Whenever Possible For individuals with cognitive impairment or memory loss. The cornerstone of this program is the use of procedural memory, a type of long-term memory that helps people remember how to do each step of a process. In most cases, procedural memory is more reliable than short-term memory or memories that include emotions.
Brain Gym Exercises
Brain Gym Exercises



What Are Brain Gym Exercises?
Brain gym exercises are simple tasks that help to stimulate brain activity and keep the mind engaged. Just like when you exercise you engage and strengthen core muscles, brain exercises stimulate blood flow to the brain and increase oxygen supply to the brain. Brain gym exercises release stress, enhance learning and development while effectively engaging the brain. Not only younger kids, but even older kids and adults can benefit from these effective yet simple brain gym exercises. And that will help the child develop good motor skills, memory and ensure effective brain Development.
Top 10 Brain Gym Exercises
- Cross Crawl:Cross crawl is a simple exercise that can be done while sitting or standing. Ask the child to touch his left elbow to his right knee and then right elbow to his left knee. This exercise is most effective when done slowly. Cross crawls helps with the bilateral integration of the left and right brain and also energizes the body.
- Number 8:This is one of the simplest brain exercises for your kid but effective nonetheless. Ask your child to draw number 8 on a book or a piece of paper repeatedly. It should be drawn with a loose hand and freely. Drawing this figure relaxes the mind and loosens up tense muscles.
- Draw with the other hand:Another simpler brain exercise is to ask the child to draw with his non dominant hand. If the child is right handed ask him to draw with his left and if the child is left handed ask him to draw with his right. Remember this has to be a fun activity so let the child draw whatever he wants and however he can.
- Brain Buttons:Ask the child to lightly press his head (between the hairline and the eyebrows) and then close their eyes and breathe. You can instruct the child to breathe in deeply and then breathe out. In between also ask the child to take a 5 second pause and then breathe in deeply. This is a rejuvenating exercise that even adults can do occasionally.
- Hook ups:For hook ups ask the child to sit in a comfortable position and then ask him to cross left ankle over his right. Stretch the arms and cross them and interlace the fingers. Then ask the child to bring his hand to his chest and keep still and breathe deeply for a minute. Hooks up help the nervous system to calm down and relax.
- Memory games:Simple games like memory games can serve as an effective brain exercise. You can bring out all the toys your kids have lay them on the floor, ask the child to close his eyes and remove a couple toys and ask the child to find out which toy is missing. This will stimulate memory function and brain activity.
- Board Games:Board games such as checkers, monopoly etc can be quite stimulating as well. You can bring out the good old ludo, carom or even the chess board can play with the kids. A competitive atmosphere and a challenging game can be a great brain gym exercise for all the members of the family, kids included.
- Scissor jumps:Jumping exercise are quite effective to promote brain functions. If you have access to a trampoline ask your kid to jump on it and while jumping ask him to cross his arms and legs. You can even do it without a trampoline just ask your kids to jump a little higher. This exercise promotes sensory development and good motor skills.
- Puzzles:Another great exercise would be to solve puzzles. Buy a puzzle that is suitable for your child’s age and sit down with the kid and help him or her solve it. It could be as simple as matching objects and as tricky as creating a picture. Choose the puzzle appropriate for your child’s age, do not tax the child buy undertaking difficult puzzles.
- Nesting and block pattern toys:Nesting toys and building blocks are easily available in the market. Encourage your child to build block patterns like making a pyramid or a cubicle this will stimulate their brain and encourage to come up with different patterns on their own. You can also buy come nesting toys that fit inside each other, dismantle them and ask the child to put it back together. This might look simple but is an excellent exercise for kids.
Brain Development
CHILD DEVELOPMENT: ACTIVITIES FOR EVERYDAY BRAIN DEVELOPMENT AND BUILDING
The first five years of life are when a child’s brain development is the fastest and when more than 700 neural connections are being formed every single second. What fosters healthy development during these critical early years?
Positive interaction is essential between children and the adults who care for them. Every time we connect with children, it’s not just their eyes that light up—it’s their brains too. Positive early experiences with adults strengthen the connections that a child builds up and help children to be eager, engaged, and ready for a lifetime of learning. This is called brain building.
Brain research has made significant discoveries about how the brain is stimulated through play. The hand and the brain need each other. Neurologically, “a hand is always in search of a brain and a brain is in search of a hand”. The use of the hands to manipulate three-dimensional objects is an essential part of brain development. According to the latest brain research, when kids play with blocks, pushes around toys and throw balls, their brains are being fertilized with constant neural growth.



Brain Development
The play personality of your child changes as per the age and development of your child:
Observe babies in the first nine months as they manipulate toys, they reach for, hold, release and suck on the toy. The focus is on manipulation as their finger muscles are developing and their brain uses all the five senses to learn.
From 9 to 18 months, children will be involved in function games with their toys which they toss, press and throw because they are curious to know what each toy can do.
18 months onwards when the brain is now geared for imagination, children indulge in imaginative play; they give a functional twist at a symbolic level to the toy or object. So a long block is used as a mobile phone or banana. This is the beginning of symbolic play which is the foundation of learning to read and write. When a child can visualize an object as having another function then the child will be able to see the word ‘c-a-t’ and visualize a cat.
So if kids don’t play, they don’t learn and that is why play is called the work of childhood.
So watch your kids play today and observe these schemas in their play. What is a schema? A schema is a repeated action in children.
- Trajectory– fascinated by the way they themselves or objects move through the air.
- Rotation– Children who just adore circles and anything that goes round
- Positioning– children who are always placing things in some kind of order
- Transporting– children who are always on the move, moving items and often carrying a bag
- Enveloping– children who like to cover themselves or objects as well as hiding
- Enclosure-children who love to surround or enclose either themselves or other objects
- Connecting– connectors simply enjoy attaching themselves or objects to other things
- Transforming-these children spend hours mixing
Yes, children thrive on play because their brains learn best with play. So even though play is a 4-letter word it is one of the best words that adults should speak around children. So tell your child to play today…and play along…it keeps you young!
CHILD BRAIN DEVELOPMENT AND BUILDING BASICS
Think about the experience of parenting as slowly releasing responsibility over time, starting when your child is in preschool. Your child should learn from an early age that you are her best advocate and cheerleader. At the same time, it’s your job to keep her safe and healthy by setting reasonable limits. Mutual respect, understanding, and cooperation guide every interaction.
Look – Even before babies can talk, they’re showing you what they’re interested in. Look into their eyes, or what catches their eye, and begin to build with your child.
Follow – Powerful moments are created when you let children lead the way and you follow by responding to their words, sounds, actions, and ideas.
Chat – It may not seem like it, but the sounds and gestures young children make are their way of communicating with you. So, talk out loud together—even if they can’t talk yet—and keep chatting as your children grow to engage them in learning about the world around them.
Take Turns – Back and forth interactions between you and your child are one of the most important ways to help development. So be sure to take turns while you’re talking, playing, or exploring with your children.
Stretch – Make the moment last longer by building on what your child says, or asking follow-up questions that expand your child’s thinking and learning. When you stretch the conversation with questions like, “What do you think about that?” or “How does that make you feel?” you’re stretching the building moments as well.
10 Important Activities To Stimulate Your Child’s Brain Development
1. Communicate With the Child
2. Introduce Books, Storytelling and Narrating Events
3. Ask Questions to Stimulate Thinking Process
4. Let Your Kids Explore – Touch, Feel, Smell, Taste
5. Music-Dance-Physical Activity
6. Building Event Memory, Associating Things & Situations
7. Independence
8. Age Appropriate Toys, Art and Craft
9. Logical Reasoning & Decision Making
10. The Most Important – Excellent Nutrition

Yoga For Autistic Children
Yoga For Autistic Children







Yoga For Autistic Children
These specific yoga poses for autism/asperser’s can help a child with ASD, child with attention and Sensory challenges These skills apply to other areas in life, ultimately helping those with ASD to lead more balanced, healthy, socially integrated, and independent lives.
- To both calm and energies their bodies
- Help them develop sensory and body awareness
- Improve focus and attention
- Improve sensory information processing
- Improve communication
- Increase their self regulation
- Enhance speech, language and motor control
- Promote social interaction
- Ease transitions
- Help them learn to monitor their anxiety levels
- Foster independence and enhance self-esteem
A List of Yoga for Kids (1-15)

1-Boat Pose:
(Balance on your buttocks with your legs up. Then rock in the water like a boat).

2-Bow Pose:
(Lie on your tummy, bend your knees, lift your chest, reach your arms back towards your toes, and hold onto your feet.)

3-Bridge Pose
(Lie on your back with your knees bent and your feet flat on the ground. Rest your arms down alongside your body, tuck your chin into your chest, and lift up your buttocks and back to create a bridge)

4-Cat Pose
(Come to an all-fours position, round your back, and tuck your chin into your chest. Pretend to be a kitty cat.)

5-Chair Pose
(Stand tall in Mountain Pose with your feet hip-width apart, bend your knees, and hop like a kangaroo)

6-Child’s Pose:
(Sit on yours heels, slowly bring your forehead down to rest in front of your knees, rest your arms down alongside your body, and take a few deep breaths.)

7-Cobbler Pose or Butterfly Pose
(Sit on your buttocks with a tall spine, bend yours legs, place the soles of your feet together, and gently flap your legs like the wings of a butterfly.)

8-Cobra Pose
(Lie on your tummy, place palms flat next to your shoulders, press into hands, lift head and shoulders off ground, and hiss like a snake.)

9-Cow Pose:
(On all fours, look up, arch your back, and open your chest.)

10-Cresent Moon Pose:
(From Mountain Pose, reach your arms up high over your head, bringing your palms together. Tilt your upper body to one side. Come back to center. Tilt your body to the other side.)

11-Dancer’s Pose:
(Stand tall in Mountain pose, stand on one leg, reach the opposite leg out behind you, place the outside of your hand, bend your torso forward with your arm out in front for balance, and arch your leg up behind you.)

12-Dancing Ganesha Pose:
(From tree pose, release your right foot and take it out front of you, with a bent right knee. Bring your hands out in front of you and hold your hands like the trunk of Ganesha, the elephant god.)

13-Dolphin Pose:
(On your hands-and-knees, bend your elbows, rest your forearms on the ground, with your palms flat, lift up your knees to straighten your legs, and look forward.)

14-Downhill skier:
(Stand tall in Mountain Pose with your feet hip-width apart and then bend your knees. Rest your elbows slightly above your knees, clasp your hands together, keep a straight spine, and look forward, pretending you are skiing down the mountain.)

15-Downward-Facing Dog Pose:
(From a standing position, bend down and place your palms flat on the ground. Step your feet back to create an upside-down V Shape with your buttocks high in the air. Straighten your legs, relax your head and neck, and look down between your legs.)
 16-Eagle Pose:
16-Eagle Pose:
(Stand tall in mountain Pose, wrap one leg around the other, bring your bent arms out in front of you, wrap your arms together the opposite way, and slightly bend your knees. Perch on a tree like eagle.)
 17-Easy Pose:
17-Easy Pose:
(Sit comfortably cross-legged, and rest your hands on your knees.)
 18-Extended Child’s Pose:
18-Extended Child’s Pose:
(Sit on your heels, slowly bring your forehead down to rest in front of your knees, place the palm of your hands flat out in front of you, and take a few deep breaths.)
 19-Extended Cat Pose:
19-Extended Cat Pose:
(Come to all fours, extend one leg out behind you, and look forward.)
 20-Extended Mountain Pose:
20-Extended Mountain Pose:
(Stand tall in Mountain Pose, Look up, and reach your arms up to the sky.)
 21-Extended side Angle Pose:
21-Extended side Angle Pose:
(From triangle Pose, bend your front leg, rest your front elbow on your thigh, and reach your other arm straight up high to sky. look up. Repeat on the other side.)
 22-Flower Pose:
22-Flower Pose:
(Come to sit on your buttocks with a tall spine, lift up your legs, balance on your sitting bones, touch the soles of your feet together, and weave your arms under your legs.)
 23-Gyan Mudra Pose:
23-Gyan Mudra Pose:
(Sit on your heels, with both hands in A-okay sign over eyes to look like the badger’s eyes.)
 24-Half Shoulder stand:
24-Half Shoulder stand:
(Lie on your back with your knees bent, feet flat on the floor, arms resting alongside your body, and chin tucked in. on an exhale, push your palms down and lift your legs straight up, making an L shape with your body. Stay in this position or squeeze your belly and raise your hips. Then, bend your elbows and place your palms on your lower back for a half shoulder stand. Pretend your feet are the flickering flames and your legs are the candlesticks.)
 25-Happy Baby Pose:
25-Happy Baby Pose:
(Lie on your back with your chin tucked in, hug your knees into your chest, then grab the outer part of your feet with both of your hands, and rock like a happy baby.)
 26-Hero Pose:
26-Hero Pose:
(Come back to rest upright on your heels, and twist your upper body like an owl. Turn your upper body one way and then the other.)
 27-Horse Stance:
27-Horse Stance:
(Stand with your legs apart, feet facing slightly outwards, bend your knees, and stand firm like a horse.)
 28-Kneeling:
28-Kneeling:
(Stand on your knees, open your chest, look up-, and reach up to the moon like a fox)
 29-Knees to chest:
29-Knees to chest:
(Lie on your back, with your arms flat alongside your body. Bend your knees and hug them close to your chest. Then circle your legs as if you are riding a bicycle upside-down.)
 30-Legs up the wall:
30-Legs up the wall:
(lie flat on your back then slowly raise your legs up straight towards the sky, making an L shape with your body. Flex your feet, keep your legs together, spread your arms out to either side, and keep your neck in a neutral position. You could rest your legs on wall instead.)
A List of Yoga for Kids (31-45)
 31-Locust Pose:
31-Locust Pose:
(Lie on your tummy, lift your chest and shoulders up, look up, clasp your hands back behind you, and glide through the water like a shark.)
 32-Lotus Mudra Pose:
32-Lotus Mudra Pose:
(Sit on your heels, stretch fingers out in front of you, and place heels of palms together in mudra to represent spines of hedgehog.)
 33-Lotus Pose:
33-Lotus Pose:
(sit with a tall spine, cross your legs, and rest the palms of your hands on your knees. Relax and breathe.)

34-Lunge Pose:
(From downward-Facing dog pose, step your right foot forward to rest on the inside of your right hand. Keep a flat back, and open your chest. Switch sides.)

35-Mountain Pose:
(Stand tall with legs hip-width apart, feet facing forward, and straighten your arms alongside your body.)

36-Pigeon pose:
(From Downward-Facing Dog pose, bring right knee to rest behind right hand, placing right foot slightly inwards, and perch like a bird.)

37-Plank Pose:
(Step back to balance on your palms and on your bent toes, keeping your arms straight and your back long and flat. Pretend to be an alligator floating in the water.)

38-Puppy Pose:
(From all-fours, take your hands out in front of you while lowering your chest towards the ground. Keep your arms straight, with your elbows raised off the ground, but rest your forehead between your extended arms. Let your spine curve naturally.)

39-Reclining Butterfly Pose:
(From lying on your back, bend your legs and bring the soles of your feet together. Take your arms out to rest at your sides. Let your whole body melt into the ground and take a few deep breaths.)

40-Resting Pose or Do nothing Pose:
(Lie on your back with your arms and legs stretched out. Breathe and rest.)

41-Riverse table top Pose:
(Come to sitting with your palms flat behind you and the soles of your feet flat in front of you, Lift your buttocks to create a table, then walk like a crab.)

42-Seated Forward Bend:
(Come to sitting on your buttocks, with your legs straight out in front of you. Bend your torso forward while keeping your spine Straight. Dangle your arms in front of you like the tentacles of an octopus)

43-Seated Twist:
(Start in staff Pose with your body in an shape. Bend your right knee and place your right foot over the other side of your left knee. Check that your spine is straight and your right foot is flat on the ground. Twist your upper body to the right. Take your left elbow to your right knee and your right hand back behind you.)

44-Shark Pose:
(Lay flat on your tummy, lift up your shoulders, and clasp your arms behind your back)

45-Staff Pose:
( Sit with a tall spine with your legs straight out in front of you. Use your hands to mimic the wheels of the train going around and around.)
A List of Yoga for Kids (46-58)

46-Standing Forward Bend Pose:
(From Mountain Pose, bend your upper Body, reach for your toes, and sway your arms like a jelly fish.)

47-Squat Pose:
(Come down to a squat, and waddle like a duck.)

48-Table Top Pose:
(Come to an all-four position with your fingers spread out and palms flat on the ground. Ensure that your back and neck are in a straight but neutral position. Your shoulders should be over your wrists and your hips should be over your knees. The tops of your feet are flat on the ground.)

49-Three Legged Dog Pose:
(Step back to hands and feet, like an upside-down “V” and gently lift one leg up at a time.)

50-Tortoise Pose:
(Sit on your buttocks with your knees bent and your feet flat on the floor. Then take your feet out wide and be you are sitting with a tall, straight spine. Slide your arms under your knees and place your hands flat on the floor outside your legs. Being forward, keeping your back and neck straight.)

51-Tree Pose:
(Stand on one leg, bend your knee, place the sole of your foot on your inner thigh, and balance. Sway like a tree.)

52-Triangle Pose:
(From a standing position, step one foot back, placing the foot facing slightly outwards, take your arms up parallel to the ground, bend at your waist, tilt your upper body, reach your front hand to gently rest on your shin, and reach your other arm straight up.)

53-Triangle Forward Bend:
(From Mountain Pose, take your right foot back, keeping your ankle bent at a 30 degree angle. Place your hands on your hips, ensuring that your back is flat and that you are looking straight ahead. Then slowly bend forward as if your hips are a hinge, keeping a flat back and a long neck. Lastly, bring your hands to your hands to your shins, ankles, or the ground, depending on what feels comfortable, all the while checking that your spine straight.)

54-Upward-Facing Dog Pose:
(Lay on your belly. Place the palms of your hands next to your shoulders and look up. Then straighten your arms and expand your chest.)

55-Warrior 1 Pose:
(Come to standing in Mountain Pose. Step one foot back, slightly angling it outwards, bend your front knee, and bring your arms straight up towards the sky, and look up.)

56-Warrior 2 Pose:
(From standing position, step one foot back, placing the foot so that it is facing slightly outwards. Take your arms up in parallel to the ground, bend your front knee, and look forward.)

57-Warrior 3 Pose:
(Stand on one leg. Extend the other leg behind you. Bend your torso forward and take your arms out in front of you to pretend that you are gliding through the water like a submarine.)

58-Wide-Legged Forward Bend:
(From Mountain Pose, step your feet out wide, bend your upper body, clasp your hands together, and pretend that your arms are the trunk of an elephant.)
Handwriting Training
Handwriting Training





Hand writing training
Handwriting is an essential skill for both children and adults even in the age of technology. Handwriting remains the primary tool of communication and knowledge assessment for students in the classroom.
Handwriting refers to a person’s writing created with a writing utensil such as a pen or pencil. The term encompasses both printing and cursive styles and is separate from formal calligraphy or typeface. It is, in essence, a visible form of a person’s voice, including pitch and tone. Because each person’s handwriting is unique, it can be used to verify a document’s writer. The deterioration of a person’s handwriting is also a symptom or result of certain diseases.
Even in this digital age, the art of handwriting has not lost its importance in education. Many schools now require that students entering kindergarten be able to write the print manuscript alphabet, as well as their own names. While cursive script writing took a backseat for several years, its usefulness has been rediscovered, and students in the upper elementary grades are again learning how to write in cursive.
Below, you will find a large assortment of various handwriting practice worksheets which are all free to print. Some of the icons link to new pages of worksheets, such as the famous quotes. Others are basic alphabet tracing. Whether you are a classroom teacher or a parent teaching kids to write at home, you’ll find plenty of great worksheets here.
Even in this age of technology, reading and marking a child’s handwritten work is still (often unfairly) the primary way that elementary teachers figure out what their pupils know.
Kids with poor handwriting may be at a disadvantage when a teacher marks their written work. They may also struggle to write creatively or even to write down answers correctly, as it takes all their concentration and effort to just get ANYTHING down on paper.
When kids struggle to write neatly and efficiently, they are often accused of being lazy, and this may affect their behavior and self esteem.
In high school years, kids who struggle with handwriting may suffer even more as they struggle to keep up with the volume of written work required.
Skills Influencing Handwriting For Kids
Handwriting for kids is influenced by many different underlying skills. I have tried to outline most of these in this article to help parents (and teachers) to better understand why a child may be struggling with handwriting.
This page gives a brief overview of the skills that can influence handwriting for kids
- Visual motor integration
- Fine motor skills
- Eye-hand co-ordination
- Spatial Perception
- Directionality
- Sensory feedback
- Orthographic coding
- Visual perceptual skills
- Motor Planning Skills
- Cognitive Skills (intellectual ability) and language ability
- Organization and problem solving skills
- Page related to hand writing for kids
These finger exercises for kids are designed to increase the dexterity and skill of the tripod fingers, with the hope of ultimately improving your child’s pencil control and handwriting. 
In order to control a pencil and develop good handwriting skills, a child’s hand muscles need to work well together.
In particular, as you can see from the picture above, three fingers: the thumb, index and middle fingers work together to control the pencil in what is called a dynamic tripod pencil grasp.
I refer to these 3 fingers as the tripod fingers.
Once your child has the hang of getting the tripod fingers to work together, the fingers should be able to move freely and easily in order to control a pencil for flowing handwriting.
Please note:
These OT finger exercises are designed for kids who have already had practice with using just their tripod fingers.
They can be used as exercises to improve handwriting.
- If your child is very young, or still tends to use 4 or 5 fingers on a pencil, first work on isolating the tripod fingers.
- If your child’s hand muscles are very weak, first work on some hand strengthening exercise.
Then head back for these finger exercises and activities to help improve pencil control and handwriting.
Keep the tripod fingers isolated
Finger ball walk
Play dough finger exercises
Mini paper crumpling
The Tripod Fingers
In all these finger exercises, your child needs to have the tripod fingers isolated.
I usually ask the child to hold a small piece of paper under the ring and little fingers.

 This arch is important as it gives stability to the joints and muscles of the hands while the tripod fingers are moving and thus reduces fatigue during handwriting.
This arch is important as it gives stability to the joints and muscles of the hands while the tripod fingers are moving and thus reduces fatigue during handwriting.
Try writing with your ring and little fingers sticking out a bit, and you can immediately feel the strain on your hand!
The kids whose hands are pictured below have not yet developed this stable arch, and all of them tire easily during handwriting tasks!
When fine motor skills are weak, it may take a child a while to get the hang of moving the tripod fingers on their own.
If your child struggles to keep the ring and little fingers down on a piece of paper, have your child hold down the fingers as shown below.
Finger Ball Walk
Introduce your child to this activity without using the tripod fingers, until they get the hang of walking the ball up and down their legs. (Or up one leg, across the tummy, and down the other leg!)
Look out for kids making grabbing movements with their hands instead of getting a WALKING movement with their fingers.
Once they have got the hang of walking their fingers, then isolate the tripod fingers as explained above.
You can also vary the size and type of ball used.
Walking DOWN the leg takes more control than walking up!
If your child has a “lazy thumb”, try using just the thumb and index fingers to walk the ball.
Play dough Finger Exercise
Use the tripod fingers to roll out small balls with a rolling movement of the fingers and small sausages with a back and forth movement of the fingers. Sausages can be easier than balls at first.
Mini Paper Crumpling
This is one of my favorite activities as it is so easy to have a box of different color papers on hand to add a 3D aspect to any picture.
- Cut small squares of crepe or tissue paper ahead of time (crepe holds its shape better) .
- Give your child one piece of paper at a time to squish a bit as shown above, using the tripod fingers of both
- Then ask your child to use just the tripod fingers of the dominant hand to one-handed ROLL the crumpled paper into a smaller, tighter ball.
- Use the balls to decorate a picture.
Here’s a quick tutorial on cutting those little squares quickly and easily…
1) Crepe paper usually comes folded up. Cut a strip about 3cm wide, right across the folds.
2) Cut the strip in half, and then snip the ends off so the folds are removed.
3) After both ends are snipped off, fan out the layers of crepe paper to separate them.
4) I like to keep a container of various colors of paper on hand, ready to use.
These finger exercises, and just about all my fine motor information and activities.
These finger exercises for kids are designed to increase the dexterity and skill of the tripod fingers, with the hope of ultimately improving your child’s pencil control and handwriting.
In order to control a pencil and develop good handwriting skills, a child’s hand muscles need to work well together.
In particular, as you can see from the picture above, three fingers: the thumb, index and middle fingers work together to control the pencil in what is called a dynamic tripod pencil grasp.
I refer to these 3 fingers as the tripod fingers.
Once your child has the hang of getting the tripod fingers to work together, the fingers should be able to move freely and easily in order to control a pencil for flowing handwriting.
Please note:
These OT finger exercises are designed for kids who have already had practice with using just their tripod fingers.
They can be used as exercises to improve handwriting.
- If your child is very young, or still tends to use 4 or 5 fingers on a pencil, first work on isolating the tripod fingers.
- If your child’s hand muscles are very weak, first work on some hand strengthening exercise.
Then head back for these finger exercises and activities to help improve pencil control and handwriting.
Keep the tripod fingers isolated
Finger ball walk
Play dough finger exercises
Mini paper crumpling
The Tripod Fingers
In all these finger exercises, your child needs to have the tripod fingers isolated.
I usually ask the child to hold a small piece of paper under the ring and little fingers.
This arch is important as it gives stability to the joints and muscles of the hands while the tripod fingers are moving and thus reduces fatigue during handwriting.
Try writing with your ring and little fingers sticking out a bit, and you can immediately feel the strain on your hand!
The kids whose hands are pictured below have not yet developed this stable arch, and all of them tire easily during handwriting tasks!
When fine motor skills are weak, it may take a child a while to get the hang of moving the tripod fingers on their own.
If your child struggles to keep the ring and little fingers down on a piece of paper, have your child hold down the fingers as shown below.
Finger Ball Walk
Introduce your child to this activity without using the tripod fingers, until they get the hang of walking the ball up and down their legs. (Or up one leg, across the tummy, and down the other leg!)
Look out for kids making grabbing movements with their hands instead of getting a WALKING movement with their fingers.
Once they have got the hang of walking their fingers, then isolate the tripod fingers as explained above.
You can also vary the size and type of ball used.
Walking DOWN the leg takes more control than walking up!
If your child has a “lazy thumb”, try using just the thumb and index fingers to walk the ball.
Play dough Finger Exercise
Use the tripod fingers to roll out small balls with a rolling movement of the fingers and small sausages with a back and forth movement of the fingers. Sausages can be easier than balls at first.
Mini Paper Crumpling
This is one of my favorite activities as it is so easy to have a box of different color papers on hand to add a 3D aspect to any picture.
- Cut small squares of crepe or tissue paper ahead of time (crepe holds its shape better) .
- Give your child one piece of paper at a time to squish a bit as shown above, using the tripod fingers of both
- Then ask your child to use just the tripod fingers of the dominant hand to one-handed ROLL the crumpled paper into a smaller, tighter ball.
- Use the balls to decorate a picture.
Here’s a quick tutorial on cutting those little squares quickly and easily…
1) Crepe paper usually comes folded up. Cut a strip about 3cm wide, right across the folds.
2) Cut the strip in half, and then snip the ends off so the folds are removed.
3) After both ends are snipped off, fan out the layers of crepe paper to separate them.
4) I like to keep a container of various colors of paper on hand, ready to use.
These finger exercises, and just about all my fine motor information and activities.
Remedial Education
Remedial Education








The Remedial Education program is an instructional program designed for students in grade 1-5 and 6-12 who have identified deficiencies in reading, writing, and maths. This program provides individualized basic skills instruction in the areas of reading, mathematics, and writing
What is Remedial Education and why are these Program in Demand?
In simple terms, a remedial program is for students who have average or higher intellectual abilities but who are not performing well in school. Typically, remedial students are not struggling because of their intellectual abilities but instead because they are struggling with one subject area like reading, writing or mathematics. Remedial program are designed to help give the students the individual attention that they need to build their skills and their confidence so that they can live up to their potential.
What is Dyslexia?
In a person with dyslexia, the brain processes written material differently. This makes it hard to recognize, spell, and decode words. People with dyslexia have problems understanding what they read. Dyslexia is a neurological and often genetic condition, and not the result of poor teaching, instruction, or upbringing. Between 5 and 15 percent of people in the United States have dyslexia.
Symptoms
Dyslexia commonly causes difficulties in word recognition, spelling, and decoding.
Dyslexia is different from delayed reading development, which may reflect mental disability or cultural deprivation. The most common signs and symptoms associated with dyslexia can be displayed at any age, but they normally present in childhood.
Childhood symptoms of Dyslexia include:
Difficulty in learning to read
Many children with dyslexia have normal intelligence and receive proper teaching and parental support, but they have difficulty learning to read.
Milestones reached later
Children with dyslexia may learn to crawl, walk, talk, and ride a bicycle later than the majority of others.
Delayed speech development
A child with dyslexia may take longer to learn to speak, and they may mispronounce words, find rhyming challenging, and appear not to distinguish between different word sounds.
Slow at learning sets of data
At school, children with dyslexia may take longer to learn the letters of the alphabet and how they are pronounced. There may be problems remembering the days of the week, months of the year, colors, and some arithmetic tables.
Coordination
The child may seem clumsier than their peers. Catching a ball may be difficult. Poorer eye-hand coordination may be a symptom of other similar neurological conditions, including dyspraxia
Left and right
The child may confuse “left” and “right.”
Reversal
They may reverse numbers and letters without realizing.
Spelling
Some children with dyslexia might not follow a pattern of progression seen in other children. They may learn how to spell a word and completely forget the next day.
Speech problems
If a word has more than two syllables, phonological processing becomes much more challenging. For example, with the word “unfortunately” a person with dyslexia may be able to process the sounds “un” and “ly,” but not the ones in between.
Concentration span
Children with dyslexia commonly find it hard to concentrate. Many adults with dyslexia say this is because, after a few minutes of non-stop struggling, the child is mentally exhausted. A higher number of children with dyslexia also have attention deficit hyperactivity disorder (ADHD), compared with the rest of the population.
Sequencing ideas
When a person with dyslexia expresses a sequence of ideas, they may seem illogical or unconnected.
Types
Dyslexia can be broken down into different subtypes, but there is no official list of dyslexia types because they can be classified in different ways.
However, the following categories are sometimes used:
Phonological dyslexia:
The person has difficulty breaking down words into smaller units, making it hard to match sounds with their written form. This is also known as dysphonetic dyslexia or auditory dyslexia.
Surface dyslexia:
The person cannot recognize a word by sight, making words hard to remember and learn. This is sometimes called dyseidectic dyslexia or visual dyslexia.
Rapid naming deficit:
The person cannot quickly name a letter or number when they see it.
Double deficit dyslexia:
The person finds it hard to isolate sounds also to name letters and numbers.
Visual dyslexia:
The person has an unusual visual experience when looking at words, although this can overlap with surface dyslexia. Sometimes people refer to “directional dyslexia,” meaning it is difficult to tell left from right. This is a common feature of dyslexia, but it is not a type.
If a person has difficulty with math learning, the correct term for this is dyscalculia. It is not dyslexia.
Stage of Development |
Dyslexia Symptoms |
|---|---|
| Before school |
|
| School Age |
|
| Teenage years and Adulthood |
|
Types of Reading Disabilities
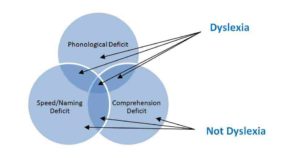
Phonological Deficit:
Difficulty decording or assembling words based on their sounds. Note that phonemic awareness is not a reading deficit per se since it involves only sounds and not letters.
Speed Naming Deficit:
Slow reading: poor use of sight. A sight word is a word that is instantly recognized by the reader: is not sounded out, and requires almost no effort to understand.
Comprehension Deficit
Poor understanding of what was just read.
Subtypes of Dyslexia
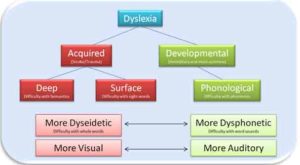
By Sensory System
Auditory Dyslexia
Auditory Dyslexia involves difficulty processing sounds of letters or groups of letters. Multiple sounds may be fused as a singular sound. For Examples the word ‘back’ will be heard as asingle sound rather than something made up of the sounds /b/ – /aa/ – /ck/. Single syllable words are especially prone to this problem
Visual Dyslexia
Visual dyslexia is defined as reading difficulty resulting from vision related problems. Though the term is a misnormer, visual problems can definitely lead to reading and learning problems.
Attentional Dyslexia
Attentional Dyslexia in which children identify letters correctly, but the letters jump between words on the page. “kind wing” would be read as “wind king”. The substitutions are not caused by an inability letters or convert them to sounds, but instead result from the migration of letters between words-the first letters of one word switches place with the first letter of another word.
By Deficit
Phonological Dyslexia
Phonological dyslexia is extreme difficulty reading that is a result of phonological impairment, meaning the ability to manipulate the basic sounds of language. The individual sounds of language become ‘sticky’, unable to be broken apart and manipulated easily.
Surface Dyslexia
A type of dyslexia characterised by difficulty with whole word recognition and spelling, especially when the words have irregular spelling sound correspondences”.
Deep Dyslexia
Deep dyslexia is an acquired form of dyslexia, meaning it does not typically result from genetic, hereditary (developmental) cause. It represents a loss of existing capacity to read, often because of head trauma or stroke that affects the left side of the brain. It is distinguished by two things:semantic errors and difficulty reading non-words.
By Time of Onset:
Developmental Dyslexia
Developmental dyslexia is not so much a type of dyslexia, it is dyslexia. In fact our definition of it would be the same as our definition of dyslexia generly: Extreme difficulty reading caused by a hereditary, brain based, Phonologic disability. So why do people use the term instead of just saying dyslexia? The simple answer is they are trying to be more specific, distinguishing ‘regular’ dyslexia from the other types of dyslexia. In particular, distinguishuing it from acquired forms of dyslexia that result from stroke or head trauma for example, which often present very differently. For more on developmental dyslexia.
Acquired Dyslexia
This type results from trauma or injury to that part of the brain that controls reading and writing. Late in life this can be the result of a tumor or stroke.
Other Dyslexia Types:
Directional Dyslexia
Directional dyslexia is distinguished by left-right confusion and tendency to become disoriented or lost. The term is also occasionally used to mean confusion with letters such as P and b or d and b, where there is confusion over the ‘direction’ of the letter. Generally, problems with direction are a symptom of dyslexia more than a sub type. Not all dyslexics have this problem.
Math Dyslexia (Dyscalculia)
Math dyslexia or dyscalculia is not, in fact, a type of dyslexia, but we included it here because the term is frequently used. According to the U.S National Center for Learning Disabilities, math dyslexia, or dyscalculia, refers to wide range of lifelong learning disabilities involving math, varies from person to person and affects people differently at different stages of life.
As with reading, when basic math skills are not mastered early, more advanced math becomes extremely difficult. Approximately half of people with dyslexia also have dyscalculia, though far less research has been conducted regarding testing, assessment and remediation.